
Part I – Fit and Healthy to Severe Aortic Stenosis
This post is kinda long (but so was the adventure it refers to) so I’ll split it into 3 installments . This part describes the developments leading up to surgery.
As I mentioned in my post “Staying Active Despite Arthritis And Two Hip Replacements”, I enjoyed several good years of a high level of activity after rehabbing from my hip surgeries
The first intimation something was wrong was when I did the senior games time trial again, and my performance was a lot worse than the previous year. I seemed to get badly out of breath after several minutes at high intensity. Over the next couple of months, this happened more than once, usually when hiking or biking up steep hills, which I knew in the past I’d been able to handle just fine.
I went to my doc for a checkup and he thought he heard a heart murmur, so he referred me to a cardiologist. Bingo! An echocardiogram (ultrasound of the heart) revealed “moderate aortic stenosis”. This means the aortic valve, which is the one leading out of the heart into the aorta, to supply blood to the entire body, was not opening enough.
Heart valves are what engineers (and plumbers) call “check valves”: they passively open under pressure to let the blood flow out, then slam shut to prevent backflow. Many times per minute, tens of thousands of times per day. The heart has an ingenious mechanism for doing this: there are 3 leaflets of tissue in a circle. They open leaving a wide area for blood flow, then slam shut to prevent backflow (“regurgitation” in medicalese).
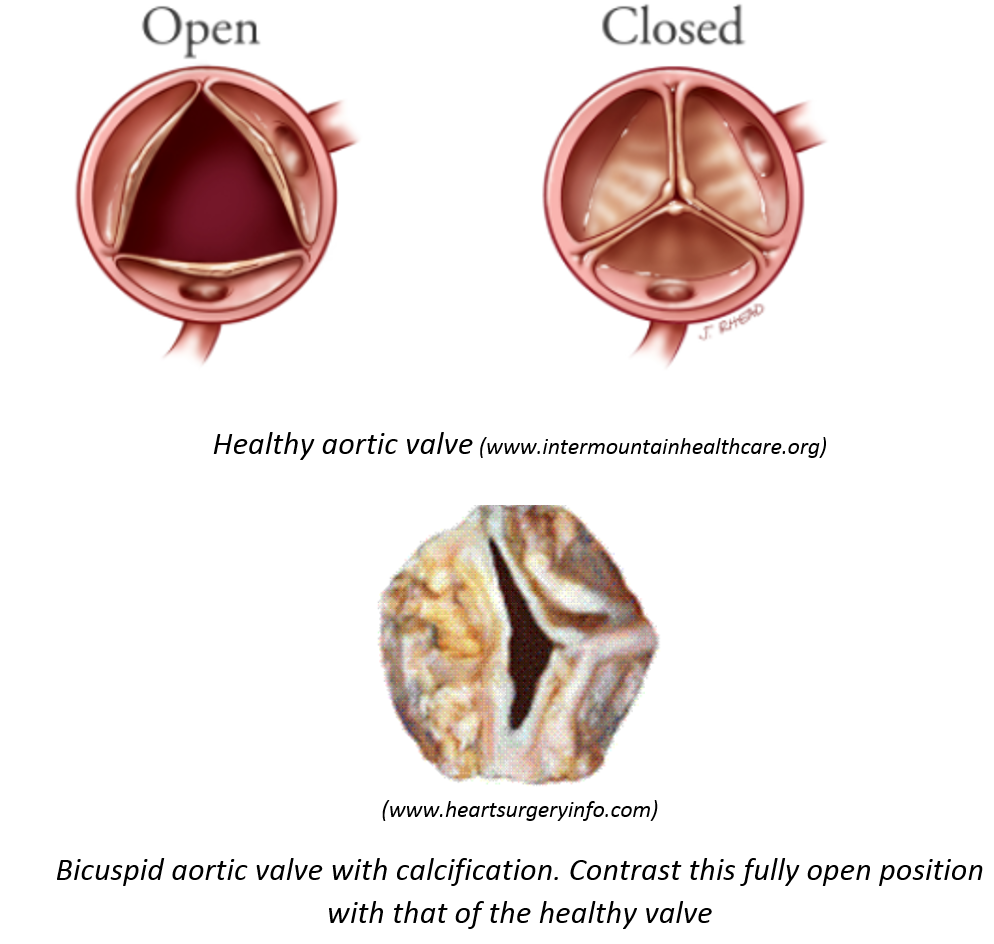
Three things can go wrong. As we age, calcium deposits form on the leaflets and they get stiffer, so the valve doesn’t open as much as it should. The second is a congenital condition where the valve has only two leaflets, known as a bicuspid valve. This does not open properly your entire life, but maybe opens enough so you get by. Then as you get older and it calcifies it goes bad more quickly than a normal valve. The first two issues cause stenosis, where the valve doesn’t open enough. The third problem is when the valve does not close properly and leaks, causing backflow, for which the medical term is regurgitation. I had stenosis but not regurgitation. My echo test could not visualize the valve well enough to tell if it was bicuspid but my cardiologist suspected it was, because I had significant stenosis already at the relatively young age of 63.
A normal aortic valve opens to about 2.5 to 4 cm2, while with moderate stenosis it is about 1 to 1.5 cm2, and it is considered severe when it goes below 1. Here’s what that amount of opening looks like:
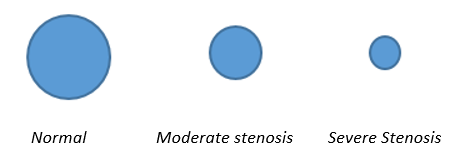
Mine was already like the middle picture, where the blood flow to my entire body had to squeeze through one of the fat straws for a Starbucks frappuccino instead of a garden hose. Later it would progress to the right picture, as small as a regular drinking straw. The first follow-up test was a treadmill stress test where they take your ekg while ramping up the speed and incline of the treadmill every couple of minutes. I ended up running briskly up a steep grade with my heart rate at 171, so I thought I had passed with flying colors. But my cardiologist noticed some arrhythmias at higher heart rate and said I could still exercise but keep it under 145. I started to monitor that with an old-school heart monitor with a chest strap. Next he sent me for a “calcium score” which gives an idea of how much calcium is in your coronary arteries. I flunked that test, which concerned him even more than the heart valve, because it meant I might have coronary artery disease.
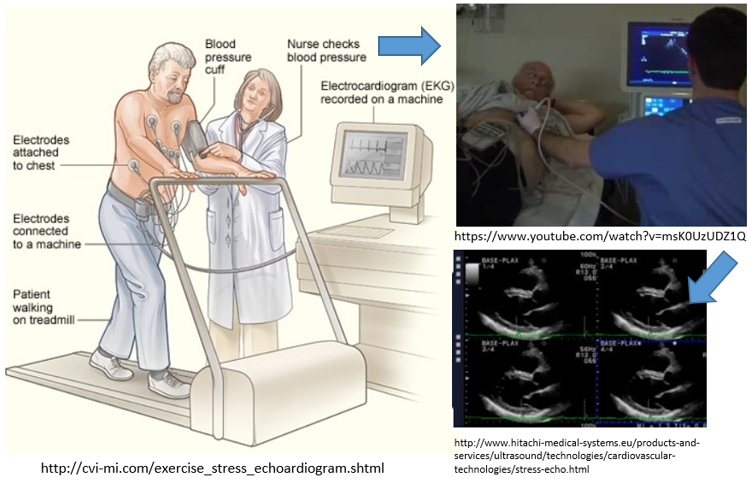
The next test was a stress-echocardiogram, an interesting experience: runninghard uphill on the treadmill again, then the tech says “ok we’re going to stop quickly” and immediately hits the stop button. I thought I was gonna fly through the front of the machine. She and the guy doing the echo then quickly got me laying down on my side while my chest was still heaving and he did a quick echo scan. The idea is to image the heart while it is working very hard. If any coronary arteries are even partially obstructed, the heart will have an abnormal shape, but mine turned out fine. This got me off the hook about the flunked calcium test.
So now I just had to follow up with regular echocardiograms every six months, which I ended up doing a couple of more times. During this period I kept exercising with the 145 limitation on heart rate, which still let me work out pretty hard, just no extended hard efforts. Short sprints and intervals were ok. I did get a repeat of the badly out of breath symptom, which I mentioned to my cardiologist, so I had to wear an “ecat” monitor (“external cardiac ambulatory telemetry”) for a couple of weeks. This continuously checked my heart rhythm day and night. When it detected an arrhythmia, it sounded an alarm and I had it upload its signal to a monitoring site. This was actually by the antiquated procedure of dialing a number and letting the gizmo whistle its tone into the phone like I was sending a fax. It seems there are still a lot of areas in medicine where high tech has not quite caught up!
I managed to set the alarm off a couple of times while exercising hard. I guess the 145 limit was no longer strict enough. My cardiologist said the ecat had detected atrial fibrillation (afib) that comes on with exercise, probably a side effect of the bum heart valve. This is significant, because afib increases your risk of stroke. So now I was no longer allowed to do vigorous exercise, only brisk walking or equivalent.
In addition, my next echocardiogram showed I’d progressed to severe stenosis. It was now time for an angiogram. This is a somewhat invasive procedure, so it is not done for assessing heart valve disease until they’re pretty sure it has progressed to severe.
They have to go in through an artery to insert a catheter for the procedure. They used to have to use the femoral artery in the groin, but if your arteries are in good enough shape they can now go in through the wrist. Fortunately that worked in my case. The angiogram showed my coronary arteries were clear, so the calcium score test had been a false alarm, which is actually quite rare.
Unblocked coronaries was the good news, the bad news was severe stenosis was confirmed, and it was time to get the valve replaced. I wanted the cardiac surgeon equivalent of Dr. Abidi so I did a lot of checking around. The best surgeon in my area turned out to be Dr. Vincent Gaudiani, who operates at El Camino hospital in Mountain View, Ca, a little over 30 miles from our house.
Valve replacement usually requires a “median sternotomy” which requires cutting your sternum completely in half. I had read about this possibly leading to long and uncomfortable rehab, so would have preferred a less invasive procedure. Dr. Gaudiani indeed does a procedure that only involves cutting the top portion of the sternum (“mini-sternotomy”) and has shorter rehab. But because I also had afib, he needed to do the “Cox-Maze III” procedure while he had me open, and this requires the full sternum cut. He assured me this was the gold standard for treating afib that accompanies aortic stenosis. Dr. Gaudiani is a great guy and our consultation with him convinced Karen and me that I would be in good hands.
We did have one other choice to make- mechanical valve vs. biological tissue valve. The mechanical valve lasts forever but you need to be on blood thinners for life. And it makes a click that can be loud enough to bother some people. That would be a bummer, “uh, doc, that click is driving me nuts. Why don’t you saw me back open and put the other valve in instead?” The tissue valves don’t require blood thinners after you leave the hospital but can calcify after about 15-20 years (or fewer if you’re unlucky) and need to be replaced.
But Dr. Gaudiani said this can be done by a minimally-invasive procedure, where a new valve is inserted via the femoral artery and deployed right inside the previous one (trans catheter aortic valve replacement, or TAVR). Or who knows what even better technique they’ll have come up with in around 15 years. So we opted for tissue, which he said would either be porcine (pig) or bovine (cow) depending on the size valve I needed. Dr. Gaudiani made it clear we had to do this asap. Once it starts progressing, stenosis gets worse quickly. I’d probably be out of breath just walking around slowly within a few months, and could be dead in a year.
Ok, no dilly-dallying. We scheduled the surgery for August 11, 2017. A bonus was that we have dear friends that live a few blocks from the hospital. It happened they would be away the time of the surgery so they let Karen stay at their house.
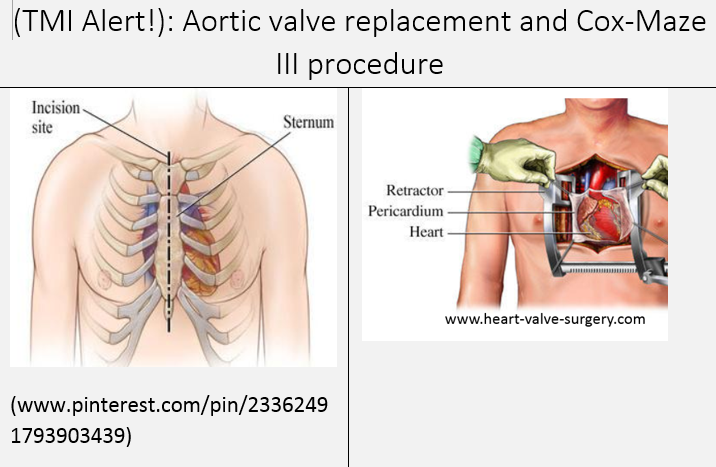
To have enough access to perform the Cox-Maze III procedure the surgeon has to cut the full length of the sternum (“median sternotomy”). Retractors pull the sternum out of the way during the procedure. The pericardium (the membrane enclosing the heart) is cut open to get to the heart. The surgeon cuts through the aorta to allow access to the valve. The old valve is removed, and a new one inserted (in my case a bovine tissue valve):

The new valve is sutured in place (there are also sutureless variations). The Cox-Maze III procedure is then performed if needed: The heart is pulled forward out of the pericardium. Talk about having your life in somebodies hands! Small nicks are made on the surface in strategic places and then sewn shut. This will leave scar tissue that disrupts the propagation of abnormal electrical signals that can cause Afib. This procedure evolved from the original procedure pioneered by Dr. James Cox [1].
I did a lot of research leading up to the surgery, and read some books on other people’s experiences. The first was Opening My Heart: A Journey from Nurse to Patient and Back Again, by Tilda Shalof. The second was The Patient’s Guide To Heart Valve Surgery, by Adam Pick. This second book also led me to Adam’s helpful website, which has lots of information on valve surgery, a surgeon finder, and many posts by patients who have undergone valve surgery. It was on Adam’s site that I found Dr. Gaudiani.
This kind of research is very useful to get an idea what to expect. The downside is you have to be careful not to get freaked out by reading about some of the other people’s experiences. Everyone is different, and “your results may vary”. For example, both Tilda and Adam talked about a lot of post-operative pain in the sternum, and the need for narcotic pain meds. Adam had to be on them long enough to be concerned with getting addicted, but was able to wean himself off in time. Because of this I showed up for surgery having read books on pain management and with self-hypnosis tapes for pain relief, which turned out not to be needed. But overall it was good for me to have a solid idea what to expect, and I went into surgery with a positive attitude.
Here is my number one tip: put yourself in a good surgeon’s hands and trust that it will go well. Do not focus on anything negative like the slight possibility of things going wrong in the surgery. Instead, focus on how great the outcome will be, and how much better you’ll feel in a couple of months after some rehab.
I also did my best to stay in as good shape as I could leading up the surgery, given my heart rate limitations. I did a lot of strength training, knowing I’d be losing strength during the period after surgery when my “sternal precautions” would limit my upper body training. From my research I found it really helps to be fit, your chances of a good outcome are higher and you’ll bounce back quicker. I remember reading one surgeon commenting “the ones who can walk a mile a day will do fine. It’s the inactive ones I worry about”. But I set my fitness bar somewhat higher than that.
(Continued in part II)
Reference


179 thoughts on “Staying Active While Aging Despite Life’s Curveballs- Heart Valve Replacement- Part I”